

Some airways are more difficult than others.
So anyone who deals with airway, knows what a video laryngoscope (hereafter VL) is. The major player in this field is the Glidescope, which has been around for quite some time.

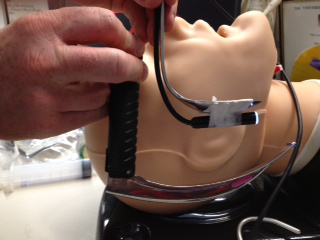
In this photo, you see the screen, a black probe-like device, and a clear plastic curved blade. The black probe has a video camera at the end of it, and it is inserted into the clear plastic blade. You then fire up the video screen, insert the probe/blade combo in the mouth, and instead if a fairly small, difficult to see set of vocal cords, you get the following:
Problem is, despite the overall fantastic-ness of these airway tools (it doubles the rate of first pass, successful intubation in emergency situations, from about 30%-ish to over 70%, and in controlled situations, first pass success approaches 95%) the stupid things are very, very spendy. Like, $2000 a pop, with the covers around $50 each. And really, folks, it’s a freaking bit of plastic. No need for that kind of coin.
Enter rfsdoc, proprietor of the PHARM: PreHospital and Retrieval Medicine blog, based out of Australia. A great site, I commend it to your review. Specific to this discussion, he is looking for a VL that costs less than $100.
He does find one, but that’s not the point of his blog post linked above. He makes one.
He uses the following equipment, pasted here from his site:
“1.Macintosh blade laryngoscope #4, disposable. I chose the Trulite version, fully disposable, $16.
2.USB waterproof endoscope, $27.
3. Windows or Apple OS laptop/tablet with USB port, use Vividtrac imaging software to display USB camera image”
Total cost, not including the laptop, $43.
Check out his finished product:

When you read his post you will see verification that it works, and that it is waterproof.
But the fun’s not over!
Again, in his words:
“But I quickly realised once again, did you really need a Macintosh blade? Would a spoon bent into the curve of a Mac blade be sufficient? YES IT WOULD!”
Top VL is spoon-based. Bottom is the Mac blade from previous, for comparison.
Any waterproof flexible video camera, similar to that linked above (say, don’t they make video cameras to look down gun barrels?). Any bendable metal with moderate rigidity. Any laptop (or cell phone, turns out) with free software, downloadable from the internet. And bam, you’ve got a $2000, incredibly useful bit of kit that would make a foundation for your grid down ICU/ER.
Yes, I know, it needs electricity. And direct laryngoscopes don’t. But off-grid electricity can be had, and part of the point of this blog is to explore what we might be able to do now, that would make a grid down scenario more survivable than Civil War era medicine.
–Grouch.

Pingback: Hogwarts: Night At The Improv | Western Rifle Shooters Association·
Good grief, I had that post up less than 10 minutes before you linked it. Quick on the draw, you are.
LikeLike
Reblogged this on Starvin Larry and commented:
Nice job-I wonder how many other things can be improvised in a grid down situation?
I’m betting a lot.
LikeLike
The amount of power needed to run a tablet charger is tiny, and the ‘scope runs on the charged tablet battery via USB power (+5vdc, very safe). A 10 pound AGM 12v battery can run lighting, ventilation fan, sterile irrigation pump and suction pump for a while (recharge on a solar panel or genset later). This kit could be tent-portable with Civilian-Off-The-Shelf parts in a shoulder bag. If the aid station was inside a van or trailer, there should be USB power-only outlets near a stand/bracket for the tablet.
If you use one of these $75 VividTrac sterile cameras on a patient, dump it back in the package for non-medical-use resale at a gun show (or gift to your armorer/plumber/mechanic). Betcha an unlimited number can be sold for $20 each in less than 30 minutes -AS-IS- “may have ick included”.
I can think of a dozen uses for a cheap peek-around-the-corner-through-a-crack camera that plugs into a cheap tablet right now.
LikeLike
I suppose I should point out that the Joint Commission has mandated that all equipment that touches a patient be subjected to “High level sterilization”–which means autoclave, or something equally nasty–before reuse. The metal Direct laryngoscope handles that anesthesia has used for decades cannot tolerate that type of abuse. So now my hospital is switching to disposable handles. The old, perfectly good metal handles are being thrown away. And let’s just say I’m not above dumpster diving.
I’d probably swipe the VividTrac with a bleach wipe before taking it to the gun show. Gotta have some standards, you know. And some diseases cannot be killed with any known method of sterilization (prion diseases, like Creutzfield-Jakob) and it’s best to just incinerate. But absent the above, yes, one man’s trash is another’s treasure.
LikeLike
Sweet. You can also use a waterproofed (with a baggie) inspection camera like this http://www.harborfreight.com/digital-inspection-camera-61839.html
LikeLike
get me a bent spoon……. stat
pure awsomeness.
Have done alot of research modifying forks knifes and spoons into retractors for improvised surgical tools but this is a new one.
Having a camera is a huge advantage. The few times I have had to intubate in the field its alwase been a messed up situation. Its one thing on a table in the OR, its another with a blast injury to the face wedged between a hesco and a displaced concrete hyway block or the 3 yr old with facial burns at night in an ambulance on a dirt road in a very hostile area or the passed out naked vomit guy on the floor of the bathroom after the paramedic paralized him but cant pass the tube.
Although intubation is not commonly needed, a camera would be a minimal addition to the laptop I already maintain in the main medicine bag.
LikeLike
Having used the Glide laryngoscope many times, performed my share of fiber optic intubations on compromised airways for whatever reason, and performed literally thousands of laryngoscopies, I would like to share some observations on this complex topic. You will require some form of suction device to remove secretions, blood, so as to actually being able to visualize the glottic opening and pass an endotracheal tube. You might want to administer some atropine, for example, if time permits, to dry up the secretions. Also, topical anesthesia and some sedation will probably be in order as well. As illustrated in your photo of that rather corpulent patient, having them in a semi recumbent position assists the operator as well as the patient. Lets not forget adequate lighting. And all of this would be in a very controlled setting, i.e., the operating room. Attempting this in the field would be difficult at best to say the least. All of this is very dependent upon the skill level and experience of the practitioner and just reading an article or two, some monographs, and watching a youtube just ain’t gonna cut it. You might want to monitor the patients’ SaO2 with an oximeter and provide some supplemental oxygen also. Finally, you should be prepared to provide positive pressure ventilation via mask in case the patient becomes obtunded for whatever reason and respirations are inadequate or absent. That of course is a very difficult task requiring excellent airway management skills, especially in that particularly large individual pictured. I am impressed with the improvised optics discussed above which can provide similar performance akin to the expensive medical devices which they are emulating.
LikeLiked by 1 person
I agree, in all respects.
The author above knows this, but allow me to be even more blunt for the readership: if you are messing with someone’s airway, and you don’t know what you are doing, you have a decent chance of killing them.
Please note that in my line of work, intubation is the most dangerous thing I do. Again, for emphasis: in the freaking ICU, full of the sickest of the sick, the most dangerous thing I do is intubate. One study (the MACOCHA Trial) argues that fully 60% of emergency intubations will have life threatening complications.
(not so in the OR, that’s a much more controlled situation, and the patients are not already dying from respiratory failure. Usually.)
This means you need to find someone for your grid down situation that has done this, in real life, in excess of 100 times minimum. And several hundred times would be better.
Got tribe?
LikeLike
Im a CRNA. The picture gave me chest pain. When I recover I’ll re-read the article.
LikeLiked by 1 person
😀
Amen!
LikeLike
Might need rib spreaders and calving gloves to get through that neck to the Crich if we can’t pass the tube……
LikeLike
I was thinking a post hole digger
LikeLiked by 1 person
RSI and other airway skills are valuable in a controlled hospital environment. Very seldom will you have the need or gear to intubate someone in the field combat environment, much less maintain those you do. One simple quick fix is the cricothyrodomy. Just be sure the patient 1. truly needs it 2. You are trained. 3. You have done it successfully before before trying it in the field. I had a troop I trained do one in Afghanistan on an officer who didn’t need it. Now only licensed medical personnel get this in my course. https://video.search.yahoo.com/video/play?p=tccc+cricothyrotomy&vid=e702d2866e8a0632388980f26da0e7f7&l=2%3A41&turl=http%3A%2F%2Fts3.mm.bing.net%2Fth%3Fid%3DWN.ckcdiyhGUGSoykVONsX0Mg%26pid%3D15.1&rurl=https%3A%2F%2Fwww.youtube.com%2Fwatch%3Fv%3DSBuoULSKMgQ&tit=Cricothyrotomy+in+Afghanistan&c=0&sigr=11bhtvorm&sigt=10tj5d16e&sigi=11v58jp8p&ct=p&age=1398119281&fr2=p%3As%2Cv%3Av&hsimp=yhs-002&hspart=mozilla&tt=b
LikeLiked by 1 person
@SFMedic,
Kudos to the personnel who can perform such tasks under the conditions you describe. That said, you do have the luxury of performing such deeds upon a rather healthy subset of the population rather than the specimen in the photo above. A cricothyrotomy in the above humanoid would be anything but easy even in the most controlled of circumstances, performed by even the most highly specialized practitioner.
LikeLike
Remember that another airway technique is a retrograde intubation, which has markedly fewer drawbacks.
Technique consists of performing a needle criche with the needle directed UP TOWARDS the head rather than towards the lungs.
Insert a guidewire (half of a wire salvaged from a heart cath traythat wasn’t used, perhaps) into the airway through the needle
Advance the guidewire until it can be retrieved from the back of the pharynx,
Place ET onto the wire, and insert it to the point that it arrives at the needle where the criche needle enters the airway.
Remove the guide wire and remove the needle and advance the tube a centimeter.with confidence that you are in the trachea, below the cords.
Just a field expedient for the tough airways…where digital ain’t an option, etc…
LikeLike
Pingback: Burns | Hogwarts School of Grid-Down Medicine and Wizardry·
Great article. These are pretty cool: http://www.inspectioncamerastore.com. I used one to look into gopher holes and and also check the status of my gutter drains.
LikeLike