
I loves me some ultrasound.
It’s quite possibly the most versatile imaging tool ever created. It can do/detect all of the following:
Transcranial dopplers for head bleeds. Estimation of elevated intracranial pressures in trauma. Retinal detachments. Abscess of neck or jaw. Guidance for central lines. Detection of clots in major vessels. Detection of poor carotid flow. Broken bones. Pneumothorax. Pulmonary edema. Pneumonia. Pleural effusions. A host of heart findings, from function to valvular problems. Inflamed gall bladders, liver damage, kidney damage, blood in the abdomen, ruptured spleen, AAAs, bladder problems. Guidance for abdominal abscess drains. Guidance for nerve blocks. DVTs. Testicular problems. Fetal ultrasounds.
And that’s just off the top of my head. There’s more, if you care to look. And they are portable.
A new, top of the line dedicated ultrasound machine for echocardiography is about, oh, $200,000.

But you don’t need that. You can get a very nice echo capable machine for around $60,000.
However, it’s many a time I’ve said to myself, wouldn’t it be sweet to just plug an ultrasound probe into my smart phone and scan away? Or my iPad? or just my laptop? Especially since many of the midrange (but perfectly functional) ultrasounds are just laptops anyway?
Yup. I’m not the first to think of that. And now, I can buy it.
 A company called Mobisante has developed ultrasounds aimed at the 3rd world/non-rich populations. Which means they will fit right in, should you be looking for something for your grid down hospital.
A company called Mobisante has developed ultrasounds aimed at the 3rd world/non-rich populations. Which means they will fit right in, should you be looking for something for your grid down hospital.
The first is a modified Microsoft/Windows smartphone:
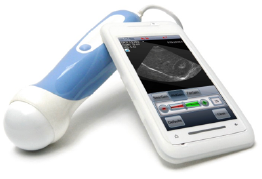
That has most of the basic capabilities, and has the advantage of being very small.
The (modified Windows) tablet has a bit more room:

As well as dedicated software, so you don’t clutter up your tablet’s memory with random YouTube videos.
The last bit is most intriguing. They will send you the software and ultrasound probe so that you can load it on your own, dedicated laptop. Whatever device you desire, although I would recommend something a bit higher end than the minimal specs.
Are they perfect? Heck no. For example, there is no dedicated echocardiography probe (that produces movies like the one at the top of this post). I don’t see that they are doppler capable. But that will be fixed, I suspect, over the next iteration of these devices. And they are selling for about 90% less than the $50,000 ones mentioned above.
—————————————————————
Disclaimer: I have not laid hands on these devices myself. They may suck beyond all compare. You should be aware that my baseline is a $70,000, dedicated ICU machine, so I would not expect these (estimated) $5000 machines to be equivalent. I have no financial interest in your purchase. As mentioned before, we’re not even an Amazon affiliate, so I really have no financial interest at all. Do your homework, and caveat emptor.
Using these things and interpreting the images are two different, moderately challenging skill sets. Any ER, ICU, cardiologist, anesthesia, or radiologist should be able to interpret the critical images. Acquisition can be done by them as well, albeit slower and with less finesse than a dedicated ultrasound tech.
Got tribe?

Yes, I love me some sonosite too….
I seem to recall about 10 years ago an ultrasound probe that would attach to a PDA….and a relatively inexpensive (like $2K) GE unit that was being advertised on TV – strapped to the back of a moped in India.
And something inexpensive for Vets. None FDA approved (not that I care).
It wold be nice if it came to fruition. Personally, I’m waiting for my medical tricorder..
LikeLike
Tricorder is on its way. http://tricorder.xprize.org/?gclid=CJKMz6qc08UCFQwMaQody5oAXw
If you haven’t spent any time at a rite aid or wallgreens lately, look at the wall near the pharmacy and see all the lab tests and devices that are over the counter now.
LikeLike
Would be interesting to see a list of alternative unofficial and unendorsed possible uses for them all.
To the op, not the paper I can find, but might be a good starting point, using ultrasound for bone fractures, though not sure if the new super cheap machines will be capable:
http://emj.bmj.com/content/17/1/22.full
LikeLike
Pingback: Hogwarts: Cheap Ultrasound Machines | Western Rifle Shooters Association·
You get what you pay for….Resolution costs money. If these tiny toys were capable of doing the job no hospital would spend tens of thousands of dollars for the higher end equipment. And the crappier the image the more subjective the diagnosis. Is it better than nothing?
Maybe….for some things. But even the top machines can miss subtle findings. And the machine is only part of the deal. A lot of MD’s think and act like they are a whiz with a US Probe……and miss obvious issues. Seen it many times…. a pronouncement of a diagnosis that was blatantly wrong and proven wrong with the proper definitive exam,
usually CT. You need a tech, one with a LOT of experience to get the most from the equipment. An experienced tech does a dozen or more exams a day and has done so for years. Again…..if the little machines were so good and the MD’s so adept there would be no work for the US department that every hospital has.
Finally….these things require maintenance and calibration….done one of two ways. Send the machine to the factory or pay a high priced Field Service Engineer to service them.
US is a tool, in the right hands for the right situations a good tool.
But that is the extent of it, it’s not the gold standard for most issues
though.
LikeLike
I agree in part, and dissent in part. But the dissent part is fairly minor.
I agree that better resolution is always desirable. For the things I do (which is about 50% of the list from the article) there is a point of decreasing return in terms of increased resolution vs capability. For other applications, that may not hold true.
I agree that the handheld machines suffer in many ways, but the most telling way is in speed of acquisition and throughput. Even if the images are the same, paying the extra money makes sense for a large facility with dozens of patients to see per day. This may or may not make sense in a grid down situation.
I would argue that the exam most dependent on a skilled tech is the echo exam, although reasonable folks might disagree. In the spirit of that argument, I benefited from doing the stats for the following publications:
http://www.ncbi.nlm.nih.gov/pubmed/20412264
http://www.ncbi.nlm.nih.gov/pubmed/21323994
Although I did not benefit by getting my name on the paper.
The overall feel from both studies was that even though the handheld device was able to obtain adequate quality images, the display on the device was too small to interpret them adequately. Once downloaded to an appropriate monitor, the source of the images became less important than the person interpreting them. For this reason, should I purchase one of the devices above, I’d be after either the tablet or using my own laptop.
I feel reasonably confident in my ability to obtain echos adequate for my needs in critical care. I’m no echo tech, however. Note that I’m looking for big stuff: effusions, severe valve problems, severe wall motion abnormalities, blown out right heart, etc. The subtle stuff I don’t attempt (with the exception of respiratory variation in flow across the mitral valve to look for hemodynamically significant pericardial effusions). I perhaps flatter myself, but I am aware of my limitations.
You are quite correct in stating that US is not typically the definitive test. CT (or MRI) typically holds that place. But CT or MRI scanners require much more resources in terms of space, electricity, and maintenance. Outside of radical change in how they operate, those are less likely to be useful in a grid-down situation.
I would miss looking at brain MRIs, should the grid go down. That was the focus of my research in graduate school, and I’ve always thought them striking.
LikeLike
In near 40 years in the radiology dept. I’ve yet to meet an MD wielding a US probe who did not consider themselves to be good at US. And a few were. But for every one that was there are plenty that think they know what they are looking at but don’t . sometimes they are so clueless they miss the ‘Ray Charles’ type of findings……like massive free fluid in the pelvis….which is a forte of US but is frequently missed by non radiologist MD’s in ER and seen on the CYA CT scan. Even most board certified radiologists will admit that while they know what they are looking at acquiring the images is the make or break part of US. The tech who does the exam determines whether or not findings are missed. In the current system where EVERYONE gets a CT regardless of whether the attending ER MD or surgeon screened with US or not it’s usually not a deal breaker. But take away CT and things gat a lot dicier.
Realistically if your going to acquire modern technology for health care you need to acquire the right people to use it. Nowhere is this more critical than imaging where the equipment has become so complex, the procedures so vital and the cost of missed findings from incorrectly performed exams. It ceased to be “button pushing” decades ago.
The biggest downside to procedures performed poorly by people who have limited training and experience is that decisions are made based on faulty assumptions. For an ER MD or surgeon to make decisions that can be life or death based on images they acquired and read should require at LEAST the same level of training, hours of supervised training and formal certification as the people who do US 40 hours a week. Otherwise you have people who took a weekend US course thinking they know what they are doing…..and actually know just enough to make them dangerous. So if you are going to wield a probe get the right training including hundreds of supervised exams and then take the board exams. If an MD is as good as they think they are they will pass if not then they might just realize they are putting patients at unnecessary risk.
LikeLike
So I have to ask how hard is it to use a US machine? I have lots of experience with a flaw detector – which is a US machine geared for finding cracks and defects in metal. Is the process for calibrating a US machine significantly harder than for an industrial machine?
I guess what I’m really asking is if I got one of those inexpensive machines would it be a steep curve to learn to use or could someone who has industrial experience make that transition quickly?
LikeLike
Things look very different on an US machine, and much of what you look for is subtle. Once those differences are in your head, then (for example) the texture of a particular organ screams out “liver!” and it becomes clearer. The thexrayboy has commented extensively on the relative inability of even trained doctors to accurately obtain and read ultrasounds, outside of radiologists. I agree with his critiques, to a point. There are non-radiologists who can read ultrasounds successfully–but those folks tend to be the type who have made it a particular research or clinical interest, and have spent the time to learn to read them. They also know their limits, and have sufficient humility to go ask when something is off. These folks are rare. I think the learning curve for you would be steep, and you would need someone to guide you in obtaining and interpreting these images.
Unlike industrial imaging, wherein you might know, more or less, where everything is, organs in the body move and are often not in the “right” place. They are frequently shadowed by bones or air pockets, making image acquisition tricky. Folks have weird anatomy up front, or anatomy messed up by surgery. That’s difficulty #1.
Difficulty #2 is more subtle. Depending on the clinical situation, an “abnormal” finding may be nothing. Or, you may find something that might be abnormal, and whether or not it is significant depends on how the patient is doing. Example: you ultrasound someone’s gall bladder and find it to be enlarged. Is this abnormal? Strictly speaking, yes. But maybe you are imaging a dude that’s 6′ 9″–the typical size doesn’t count for him. Or perhaps you’ve got a guy with stomach problems and his gall bladder has reacted to those problems by enlarging. No way to tell. Radiologists end many a read with the phrase “correlate clinically”, which means–go see your patient and figure out if he is having clinical pain or problems that may be caused by the gall bladder. That makes all the difference in the world.
Hope that helps.
LikeLike
Thanks that does help. I’ve thought for about a year of getting one of the laptop machines they sell on ebay and figured that while I couldn’t interpret the results I could at least run it and maintain it if we had a doctor join our group. I didn’t think about needing a separate person to do the analysis for the doctor.
I work oil patch and I have a moderate amount of 1st aid skills which thankfully I have not had to use all that frequently. I consider myself competent to stabilize a person till actual medical staff (paramedics etc) get to them. I’m trying to look at gear or skills I can add to make me more useful in a major emergency but most of those classes are not the evening and weekend kind of classes so I’ve been reading your site for a couple months and trying to think of ways to “adapt” my other skills to medical use.
LikeLike
I had a thought, years ago the rep for our UT supplies told me that the gel we use is “nearly identical” to the gel used for US, he explained the difference was in guaranteed purity and possible additives. Does anyone have the ingredient list for US gel? They look identical and the UT gel is used for doing US on metal structures. I just know from talking to the rep that the price is way cheaper on the commercial vs. medical side and in a post grid situation any company that advertises as doing NDE (non- destructive examination) could be a source for gel that could be used for US if someone still had a machine functioning.
I can post the MSDS for the commercial gel I use if that would be helpful?
LikeLike
As I understand it it’s pretty much just ky jelly.
The main point as I’m sure you’re aware is to eliminate the air gap so you can get good transmission of the sound waves. Just about anything that has that gel consistency to stick around should work with varying effectiveness. You could try it yourself with your job–just grab some hand lotion or something and try it to see what changes when you have some spare time.
Probably something Grouch or someone could write a nice little paper on–run a few different substances and discuss the differences and then make suggestions for how to select a substitute in an emergency situation and all that. Might talk to my community college–be a fun class project for such too.
LikeLike
With an industrial UT machine I will warn you that the couplant you use makes a noticeable difference in the thickness readings, we recalibrate our machines to a test block as soon as we open a new batch of gel or even if the room temp changes enough or if the temp of the item we are scanning changes more than a few degrees.
I’ve used hand lotion once as an experiment to show a class of kids I was demonstrating too; also did water, KY jelly and toothpaste. In the field we use white grease for certain pieces of equipment that are above 100C as the regular gel boils at that temp.
The big think is it has to be a consistent viscosity with no air to work, I know the brand we use is safe for skin contact and isn’t poisonous to ingest.
LikeLiked by 1 person
You can get ultrasound machines in pretty much any shape or size today. We have a couple of handheld ULS machines in our ER, I think they are from GE – approx. size of a small tablet.
And the price mentioned in the article is for new. We have, as far as I know, never made a 200k buy of a ULS. If you do like us – buying refurbished, you can get 3 ULS machines for the same price – or more. We have both cardiology machines, portables and handheld. I think all refurbished, except handheld. Cant remember. We buy at lbnmedical.com, fyi.
Kind regards,
Dr. Vogel
LikeLike