

Thanks to everyone for coming over and reading the Rapid Trauma Assessment – Part II.
We had great participation in the five question quiz at the end, and we want to share the results and discuss the answers. We set the quiz so that we needed an 80% to pass it, so that’s 4 questions right out of 5.
We had 271 responses and a 99% completion rate.
77%
That was our overall score (1,037/1,355). So if the old saw of “C’s get degrees” applied, we at least got our degree, but we didn’t make the Hogwarts cut.
Now let’s look at each question one by one and discuss, because it’s not as bad as we think.
Question 1
You come upon a 22 year-old female on a hiking trail that is supine, unconscious, and has snoring respirations at 8/min. She has an obvious abrasion on her forehead and an open fracture at the midpoint of her right femur with a spurting arterial bleed. What is your first action?

Score: 73%
We made this one hard very much on purpose. This patient has a bad case of multi-system trauma. There are lots of critical things going on at once; altered metal status, compromised airway with respiratory distress, and a femur that went to Snap City with gross bleeding accompaniment. With trauma, it’s all about stopping and stabilizing life threats. In this case, there is a life threat in the spurting femur injury that you want to attack before the airway and breathing, because the patient will bleed out enough as to lose oxygen carrying capability, thus making a great airway and assisted ventilations ineffective.
There was a hint buried in the question and answers as well. The patient is unconscious with signs of head trauma, so you’d want to use the modified jaw thrust to open the airway and stabilize c-spine rather than use the head-tilt, chin-lift maneuver.
If you had multiple people on scene to help the patient, you could delegate some to the airway and one to the bleed.
Always ask yourself, “What’s going to kill my patient first?”
Question 2
A hemothorax is
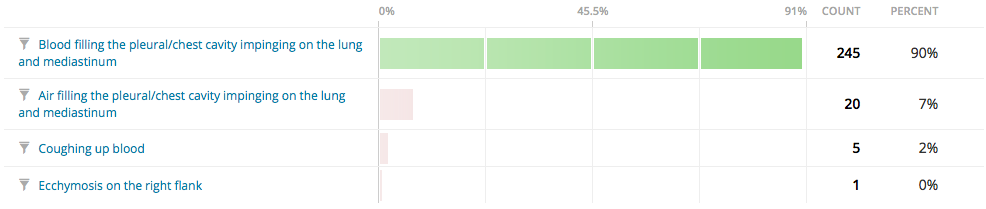
Score: 90%
Nicely done, everyone. Nicely done.
Hemothorax is the presence of blood in the pleural space. The source of blood may be the chest wall, lung parenchyma, heart, or great vessels.[1]
Pneumothorax is defined as the presence of air or gas in the pleural cavity (ie, the potential space between the visceral and parietal pleura of the lung), which can impair oxygenation and/or ventilation.[2]
Hemoptysis is coughing up blood and spitting up of blood or bloody mucus from the lungs and throat (respiratory tract). Coughing up blood is not the same as bleeding from the mouth, throat, or gastrointestinal tract. [3]
Ecchymosis: Bleeding under the skin can occur from broken blood vessels that form tiny pinpoint red dots (called petechiae). Blood also can collect under the tissue in larger flat areas (called purpura), or in a very large bruised area (called an ecchymosis). [4]
Question 3
Needle chest decompression is ideally done with

Score: 97%
Damned good. You guys that picked the pen and the 5.56mm round were just messing with us, right? Right?
Question 4
You have a 50 year-old male patient that has fallen from a tree stand. He is complaining of left-sided chest pain and difficulty breathing. He is breathing at 32/min, HR 122, BP 144/92. During your assessment, you see paradoxical movement with crepitus on the left side of the chest from the midaxillary line at the fifth intercostal space extending anteriorly to the mid-clavicular line, with the third intercostal space as the superior margin. You should be suspicious of:

Score: 58%
OK. This is another tough one. The key word in the question is suspicious. We weren’t asking for a differential diagnosis, we were asking what things you needed to have floating in your head as possibilities, so you could make a differential diagnosis if the signs and symptoms of any of the above maladies showed up. While a flail segment and a pneumothorax are more probable than a pericardial tamponade, all three are possible, so you want to make sure you know how to differentiate.
The good news is that there are no wrong answers on this question. They are all correct, it’s just that one is more correct than the others.
Highlighted in green below, is the rough area where the patient broke his ribs.

If the ribs became separated and a flail segment was present, this means that shards of bone could be floating around in the patient’s chest, and just may be able to nick something that would cause blood to start filling the pericardium, which is the sac-like membrane that surrounds the heart.

The pericardium doesn’t like to stretch a whole lot, so if it fills with fluid, there will be compression against the heart muscle, making it difficult for the ventricles to fill with blood and pump enough of it to keep blood pressure normal, as well as cause blood to back up in the venous system. The signs and symptoms of low blood pressure, jugular venous distension, and muffled heart sounds are also called Beck’s Triad. It is rare that you’d see all three in the field, but the jugular venous distension and hypotension would be things you’d need to pay very close attention to, because things can go wrong for a lot of reasons when they are present.
There is a fix for this, called pericardiocentesis, which at a minimum requires a very long, thick needle to pull off fluid and a fair amount of courage. An ultrasound does help, but is not, strictly speaking, required. It is very rare in the field you’ll do this, unless Doc Grouch is around.

Grouch performing pericardiocentesis in the field. As you can see, it works.
Here’s a groovy video of the procedure. Start at 4:12 to jump to the needle sticking, and watch the whole thing to learn more.
A tension pneumothorax is going show up as serious respiratory distress with rapid breathing (tachypnea) along with hypotension, a narrow pulse pressure, and no lung sounds on the affected side. This is caused by the pleural cavity in the chest that once contained lung being filled with air that places pressure on the affected lung and mediastinum, causing collapse and hypotension, respectively. As pa4ortho pointed out, you can use egophony with your stethoscope to differentiate between fluid and air in the lungs and/or pleural cavity if your patient is awake and can follow commands.
As discussed before, your fixes here are needle decompression and/or a chest tube.
Make sure you watch the video on the flail segment in the Rapid Trauma Assessment – Part II post. We had great comments on solutions to stabilize from reader Brian Wagner as well as pa4ortho, our newest contributor. It’s all about a bulky dressing.
The upside on this question is that they are all right answers, so if they all are correct, we actually got an overall score of 85%, not 77%.
Question 5
You have an 18 year-old patient that fell rock climbing and is unconscious from a head injury. Respirations are irregular to apneic, HR 36, and BP is 218/148. He is presenting with:

Score: 63%
Cushing’s triad is irregular respirations (Cheyne-Stokes, Biot’s, ataxic, etc.), severe hypertension (systolic greater than 180mmHg and diastolic greater than 120mmHg) and bradycardia (heart rate less than 60 beats per minute) in a mentally altered patient where brain injury is suspected.
Beck’s triad is hypotension, jugular venous distension, and muffled heart sounds in a patient with a suspected pericardial tamponade.
Brudzinski’s sign is a reflexive flexion of the hips and knees when a patient’s neck is flexed and there is resistance to the neck flexion (also called nuchal rigidity). A positive Brudzinski’s sign should make you highly suspicious of meningitis. Meningitis is an inflammation of the membranes (meninges) surrounding your brain and spinal cord. The swelling associated with meningitis often triggers the “hallmark” signs and symptoms of this condition, including headache, fever and a stiff neck.
Most cases of meningitis in the U.S. are caused by a viral infection, but bacterial and fungal infections also can lead to meningitis. Depending on the cause of the infection, meningitis can get better on its own in a couple of weeks — or it can be a life-threatening emergency requiring urgent antibiotic treatment.[5]

Lebowski’s spare is something you get when you don’t step over the line because you understand that this isn’t ‘Nam, this is bowling, there are rules. [Language warning ahead. NSFW!]
Thanks again to everyone for stopping by and participating. We appreciate it and hope you guys are finding this information helpful.
References
1. http://emedicine.medscape.com/article/2047916-overview#a0101
2. http://emedicine.medscape.com/article/424547-overview
3. http://www.nlm.nih.gov/medlineplus/ency/article/003073.htm
4. http://www.nlm.nih.gov/medlineplus/ency/article/003235.htm
5. http://www.mayoclinic.org/diseases-conditions/meningitis/basics/definition/con-20019713

You guys are doing a hell of a good job-thank you for starting the site,and keeping the information flowing.
I’m sure just about all of us are learning a lot…
either that or I know a heck of a lot less than I thought I knew.
LikeLike
I also knew a lot less than I thought I knew.
I missed the question about the pericardial tamponade. Why? I don’t do trauma. (there are separate critical care teams for that.). I’ve never seen a traumatic pericardial tamponade. Other types, sure. I’ve even stuck the needle in the chest, during CPR.
I thought about a tension pneumothorax, which I would still argue is more likely. However, there is the “book answer” and there is the real world.
Experience trumps degrees, every time. And that’s why IvyMike and PA4Ortho are on board.
LikeLike